|
|
Projects
Malaria Drug Resistance (MDR)
|
|
OVERVIEW |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Malaria Drug Resistance (MDR) laboratory conducts comprehensive surveillance
of antimalarial drug resistance throughout Kenya through in vitro susceptibility testing,
in vivo efficacy studies, and genetic analysis of
Plasmodium falciparum populations. MDR’s efforts provide invaluable
epidemiological data, which directly supports the scientific objectives of
KEMRI/USAMRD-K and its partners, and provides timely information to U.S.
Department of Defense and Kenya Ministry of Health in order for these agencies
to make informed malaria policy decisions. This exceptional quality essay writing services provide targeted support to students for essay writing and homework, featuring expert advice and a broad array of resources. It focuses on improving students' academic performance and enhancing their writing skills.
MDR is comprised of three sections,
the in vitro parasite culture laboratory,
in vivo efficacy
laboratory, and the molecular genetics and bioinformatics laboratory, and has a
staff of one uniformed service officer, one medical officer, one doctoral level
scientist, three master’s level scientists, five laboratory technicians, and
four graduate students. This essay service WritePaper offers students fast and reliable online assistance with their studies and writing assignments. Through personalized support, it helps improve understanding and writing skills, ensuring students can meet their deadlines and succeed academically with greater ease.
 |
 |
|
|
|
|
|
|
|
|
|
|
|
MDR team |
|
|
|
|
|
|
|
|
MISSION |
|
|
|
|
|
|
|
1. To use in vitro drug susceptibility tests, in vivo efficacy studies, and next
generation sequencing as comprehensive surveillance tools to monitor for the
emergence and spread of antimalarial drug resistance.
2. To support our partners
and collaborators, with a focus on testing new antimalarial compounds.
3. To provide comprehensive surveillance data to the USAFRICOM Commander for
policy decisions and prioritization of U.S. DoD product development for the
warfighter.
4. To provide useful data on prevalence and patterns of drug resistant parasites
and advise the Kenya Ministry of Health on malaria treatment and prevention
strategies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MDR LABORATORY CAPABILITIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• MDR operates 7 field sites in strategic locations throughout Kenya
representing the different malaria endemicities.
• MDR acquired next generation sequencing platforms including the Illumina
MiSeq, ABI 3500xL Genetic Analyzer, and Agena MassARRAY platform, which allows
for the genotyping for the 30 different drug resistance markers as well as whole
genome sequencing of Plasmodium falciparum to determine the population
structures.
• The MDR in vitro laboratory has a Biomek FXp automated liquid handling
workstation with dual multichannel, incubators for parasite culture, two level
II biological safety cabinets, and liquid nitrogen freezers. The in vitro
laboratory measures parasite survival after drug exposure at various
concentrations in order to ascertain resistance patterns.
• MDR utilizes quantitative PCR for Plasmodium species analyses and has an
established PCR malaria diagnostic system with a turn-around time of 2 hrs for
referral of diagnosis of malaria infection.
• MDR acquired the expertise to perform the novel ring stage survival assay to
specifically test for low-level artemisinin resistance during initial
antimalarial treatment.
• MDR mastered the technique for isolating single clones from samples obtained
from naturally infected individuals, which are helpful for use for challenge
studies.
• MDR maintains an archive of more than 20,000 Plasmodium falciparum field
isolates collected since 1991. |
|
|
|
|
|
Download
the PDF |
|
|
|
Publications.
1.
Ingasia LA, Cheruiyot J,
Okoth SA, Andagalu B, Kamau E. (2015). Genetic variability and population
structure of Plasmodium falciparum parasite populations from different malaria
ecological regions of Kenya. Infect Genet Evol. 2015 Oct 12. pii:
S1567-1348(15)30013-7.
2.
Achieng, AO. Muiruri, P.,
Ingasia LA., Opot, BH., Juma, DW., Yeda, R., Ngalah, BS., Ogutu, BR., Andagalu
B., Akala HM., Kamau E. (2015). Temporal trends in prevalence of Plasmodium
falciparum molecular markers selected for by artemether-lumefantrine treatment
in pre-ACT and post-ACT parasites in western Kenya. International Journal for
Parasitology: Drugs and Drug Resistance, Volume 5, Issue 3, December 2015, Pages
92–99
3.
Ngalah BS, Ingasia LA,
Cheruiyot AC, Chebon LJ, Juma DW, Muiruri P, Onyango I, Ogony J, Yeda RA,
Cheruiyot J, Mbuba E, Mwangoka G, Achieng AO, Ng'ang'a Z, Andagalu B, Akala HM,
Kamau E. (2015). Analysis of major genome loci underlying artemisinin resistance
and pfmdr1 copy number in pre- and post-ACTs in western Kenya. Sci Rep. 6;5:8308
4.
Ingasia LA, Akala HM,
Imbuga MO, Opot BH, Eyase FL, Johnson JD, Bulimo WD, Kamau E. (2015). Molecular
characterization of the cytochrome b gene and in vitro atovaquone susceptibility
of Plasmodium falciparum isolates from Kenya. Antimicrob Agents Chemother.
59(3):1818-21.
5.
Kamau E, Campino S,
Amenga-Etego L, Drury E, Ishengoma D, Johnson K, Mumba D, Kekre M, Yavo W, Mead
D, Bouyou-Akotet M, Apinjoh T, Golassa L, Randrianarivelojosia M, Andagalu B,
Maiga-Ascofare O, Amambua-Ngwa A, Tindana P, Ghansah A, MacInnis B, Kwiatkowski
D, Djimde AA. K13-Propeller Polymorphisms in Plasmodium falciparum Parasites
From Sub-Saharan Africa. J Infect Dis. 2014.
6.
Ghansah A, Amenga-Etego
L, Amambua-Ngwa A, Andagalu B, Apinjoh T, Bouyou-Akotet M, Cornelius V, Golassa
L, Andrianaranjaka VH, Ishengoma D, Johnson K, Kamau E, Maïga-Ascofaré O, Mumba
D, Tindana P, Tshefu-Kitoto A, Randrianarivelojosia M, William Y, Kwiatkowski
DP, Djimde AA. (2014). Monitoring parasite diversity for malaria elimination in
sub-Saharan Africa. Science. 2014 Sep 12;345(6202):1297-8. doi:
10.1126/science.1259423.
7.
Kamau E, Akala HM,
Achieng AO, Yeda R, Ingasia LA, Cheruiyot AC, Juma DW, Okudo C, Omariba D,
Muriuki C, Owiti EA, Omondi P, Otedo A, Andagalu B, Ogutu B. (2015) Case Report
of Attenuated-Responsiveness to Coartem® in Western Kenya. IJMPCR 2(1): 5-9,
2015
8.
Namukobe J, Kiremire BT,
Byamukama R, Kasenene JM, Akala HM, Kamau E, Dumontet V. (2014). Antiplasmodial
compounds from the stem bark of Neoboutonia macrocalyx pax. J Ethnopharmacol.
13;162:317-22. doi: 10.1016/j.jep.2014.12.018. Epub 2014 Dec 19.
9.
Akala HM, Achieng AO,
Eyase FL, Juma DW, Ingasia L, Cheruiyot AC, Okello C, Omariba D, Owiti EA,
Muriuki C, Yeda R, Andagalu B, Johnson JD, Kamau E. (2014). Five-year tracking
of Plasmodium falciparum allele frequencies in a holoendemic area with
indistinct seasonal transitions. J. Multidiscip. Healthc. 2014 Nov
6;7:515-23.
10.
Achieng AO, Ingasia LA,
Juma DW, Cheruiyot AC, Okudo CA, Yeda RA, Cheruiyot J, Akala HM, Johnson J,
Andangalu B, Eyase F, Jura WG, Kamau E. (2014). Doxycycline reduced in vitro
susceptibility in Plasmodium falciparum Kenyan field isolates is associated with
PftetQ KYNNNN sequence polymorphism. Antimicrob Agents Chemother. 2014 Jul 28.
pii: AAC.02788-13.
11.
Juma DW, Omondi AA,
Ingasia L, Opot B, Cheruiyot A, Yeda R, Okudo C, Cheruiyot J, Muiruri P, Ngalah
B, Chebon LJ, Eyase F, Johnson J, Bulimo WD, Akala HM, Andagalu B, Kamau E.
(2014). Trends in drug resistance codons in Plasmodium falciparum dihydrofolate
reductase and dihydropteroate synthase genes in Kenyan parasites from 2008 to
2012. Malar J. 2014 Jul 2;13(1):250.
12.
Cheruiyot J, Ingasia LA,
Omondi AA, Juma DW, Opot BH, Ndegwa JM, Mativo J, Cheruiyot AC, Yeda R, Okudo C,
Muiruri P, Bidii NS, Chebon LJ, Angienda PO, Eyase FL, Johnson JD, Bulimo WD,
Andagalu B, Akala HM, Kamau E. (2014). Polymorphisms in Pfmdr1, Pfcrt and Pfnhe1
Genes are Associated with Reduced in vitro Activities of Quinine in Plasmodium
falciparum Isolates from Western Kenya. Antimicrob Agents Chemother.
58(7):3737-3743
13.
Wahome MM, Nyataya JN,
Akala HM, Awinda GO, Mutai BK, Waihenya R, Kamau E, Omar SA, Waitumbi JN (2014)
Chloroquine tolerance in 3D7 strain of P. falciparum was associated with change
in allelic structure and not Pfcrt and Pfmdr1 transporter genes nor DNA
methylation. American Journal of Biology and Life Sciences 2(5): 100-107
14.
Derese, S, Barasa L,
Akala HM, Yusuf AO, Kamau E, Heydenreich M, Yenesew. A. (2014).
4'-Prenyloxyderrone from the stem bark of Millettia oblata ssp. teitensis and
the antiplasmodial activities of isoflavones from some Millettia species.
Phytochemistry Letters 8 (2014) 69–72
15.
Atilaw Y, Heydenreich,
M., Ndakala A., Akala HM, Kamau E, Yenesew A . 3-Oxo-14α,15 α-epoxyschizozygine:
A new shizozygane indoline alkaloid from Schizozygia coffaeoides. Phytochemistry
Letters. 2014
16.
Omole RA, Gathirwa J,
Akala H, Malebo HM, Machocho AK, Hassanali A, Ndiege IO. (2014).
Bisbenzylisoquinoline and hasubanane alkaloids from Stephania abyssinica (Dillon
& A. Rich) (Menispermeceae). Phytochemistry. 103:123-8. doi:
10.1016/j.phytochem.2014.03.026. Epub 2014 Apr 12.
17.
Andagalu B, Mativo J,
Kamau E, Ogutu B. (2014) Longitudinal study on Plasmodium falciparum gametocyte
carriage following artemether-lumefantrine administration in a cohort of
children aged 12-47 months living in Western Kenya, a high transmission area.
Malar J. 2014 Jul 9;13:265. doi: 10.1186/1475-2875-13-265. PMID: 25007860
18.
Induli M, Gebru M,
Abdissa N, Akala H, Wekesa I, Byamukama R, Heydenreich M, Murunga S, Dagne E,
Yenesew A. (2013). Antiplasmodial quinones from the rhizomes of Kniphofia
foliosa. Nat Prod Commun. 8(9):1261-4
19.
Kamau E, Alemayehu S,
Feghali KC, Komisar J, Regules J, Cowden J, Ockenhouse CF. (2014) Measurement of
parasitological data by quantitative real-time PCR from controlled human malaria
infection trials at the Walter Reed Army Institute of Research. Malar J. 2014
Jul 28;13:288. doi: 10.1186/1475-2875-13-288.
20.
Eyase FL, Akala HM,
Ingasia L, Cheruiyot A, Omondi A, Okudo C, Juma D, Yeda R, Andagalu B, Wanja E,
Kamau E, Schnabel D, Bulimo W, Waters NC, Walsh DS, Johnson JD. (2013). The Role
of Pfmdr1 and Pfcrt in Changing Chloroquine, Amodiaquine, Mefloquine and
Lumefantrine Susceptibility in Western-Kenya P. falciparum Samples during
2008-2011. PLoS One.8(5)
21.
Ochieng CO, Manguro LA,
Owuor PO, Akala H. (2013). Voulkensin C-E, new 11-oxocassane-type diterpenoids
and a steroid glycoside from Caesalpinia volkensii stem bark and their
antiplasmodial activities. Bioorg Med Chem Lett. 15;23(10)
22.
Kerubo LO, Midiwo JO,
Derese S, Langat MK, Akala HM, Waters NC, Peter M, Heydenreich M. (2013)
Antiplasmodial activity of compounds from the surface exudates of Senecio
roseiflorus. Nat Prod Commun. 8(2):175-6.
23.
Endale M, Ekberg A, Alao
JP, Akala HM, Ndakala A, Sunnerhagen P, Erdélyi M, Yenesew A. 2012.
Anthraquinones of the Roots of Pentas micrantha. Molecules. 18(1):311-21.
24.
Owuor BO, Ochanda JO,
Kokwaro JO, Cheruiyot AC, Yeda RA, Okudo CA, Akala HM. (2012) In vitro
antiplasmodial activity of selected Luo and Kuria medicinal plants. J
Ethnopharmacol. 144(3):779-81.
25.
Endale M, Ekberg A, Akala
HM, Alao JP, Sunnerhagen P, Yenesew A, Erdélyi M. (2012)
Busseihydroquinones A-D from the Roots of Pentas bussei. J Nat Prod.
75(7):1299-304.
26.
Yenesew A, Akala HM,
Twinomuhwezi H, Chepkirui C, Irungu BN, Eyase FL, Kamatenesi-Mugisha M, Kiremire
BT, Johnson JD, Waters NC. (2012). The antiplasmodial and radical scavenging
activities of flavonoids of Erythrina burttii. Acta Trop. 123(2):123-7. doi:
0.1016/j.actatropica.2012.04.011.
27.
Akala, H.M., Lee, P., and
Johnson, D.J. 2012. In vitro Module, WWARN 2011. P.falciparum drug sensitivity
assay using SYBR® Green I Assay Technique WWARN Procedure WWARN INV08: Procedure
http://www.wwarn.org/learning/procedures/INV08;
http://www.wwarn.org/sites/default/files/WWARN%20Procedure_INV08.pdf
28.
Ochieng' CO, Owuor PO,
Mang'uro LA, Akala H, Ishola IO. (2012). Antinociceptive and antiplasmodial
activities of cassane furanoditerpenes from Caesalpinia volkensii H. root bark.
Fitoterapia 83 (2012) 74–80.
29.
Eyase FL., Akala, HM,
Johnson, JD, Walsh DS. (2011) Inhibitory activity of ferroquine, versus
chloroquine, against western Kenya Plasmodium falciparum field isolates
determined by a SYBR Green I in vitro assay. Am J Trop Med Hyg., 85(6), pp.
984–988
30.
Endale M, Alao JP, Akala
HM, Rono NK, Eyase FL, Derese S, Ndakala A, Mbugua M, Walsh DS, Sunnerhagen P,
Erdelyi M, Yenesew A. (2011) Antiplasmodial Quinones from Pentas longiflora and
Pentas lanceolata. Planta Med. 78(1):31-5.
31.
Fukuda MM, Klein TA,
Kochel T, Quandelacy TM, Smith BL, Villinski J, Bethell D, Tyner S, Se Y, Lon C,
Saunders D, Johnson J, Wagar E, Walsh D, Kasper M, Sanchez JL, Witt CJ, Cheng Q,
Waters N, Shrestha SK, Pavlin JA, Lescano AG, Graf PC, Richardson JH, Durand S,
Rogers WO, Blazes DL, Russell KL; AFHSC-GEIS Malaria and Vector Borne Infections
Writing Group, Akala H, Gaydos JC, DeFraites RF, Gosi P, Timmermans A, Yasuda C,
Brice G, Eyase F, Kronmann K, Sebeny P, Gibbons R, Jarman R, Waitumbi J,
Schnabel D, Richards A, Shanks D. (2011). Malaria and other vector-borne
infection surveillance in the U.S. Department of Defense Armed Forces Health
Surveillance Center-Global Emerging Infections Surveillance program: review of
2009 accomplishments. BMC Public Health. 11 Suppl 2:S9.
32.
Akala, HM., Eyase, FL.,
Cheruiyot, AR., Omondi, AA., Ogutu, BR., Waters, NC., Johnson, JD., Polhemus,
ME., Schnabel, DC., and Walsh, DS. (2011) Anti-malarial drug sensitivity profile
of western Kenya plasmodium falciparum field isolates determined by a SYBR green
I in vitro assay, and molecular analysis. Am J Trop Med Hyg 2011 85 (1);Pg 34 –
41
33.
Juma P. W., Akala HM.,
Eyase FL., Muiva LM., Heydenreich, M., Okalebo FA., Gitu PM., Peter MG., Walsh
D., Imbuga M., Yenesew A. (2011) Terpurinflavone: An antiplasmodial flavone from
the stem of Tephrosia Purpurea, Phytochemistry Letters 4 (2011) 176–178
34.
Spalding, MD., Eyase,
FL., Akala, HM., Bedno, S., Prigge, ST., Coldren, RL., Moss, WJ., and Waters,
NC. (2010). Increased prevalence of the pfdhfr/phdhps quintuple mutant and rapid
emergence of pfdhps resistance mutations at codons 581 and 613 in Kisumu, Kenya.
Malaria Journal 2010, 9:338
http://www.malariajournal.com/content/9/1/338
35.
Akala H. M., Waters N.
C., Yenesew A., Wanjala C., Ayuko Akenga T. (2010). In vitro antiplasmodial and
cyclin- dependent protein kinase (Pfmrk) inhibitory activities of selected
flavonoids in combination with chloroquine (CQ) and artemisinin. Research in
Pharmaceutical Biotechnology Vol. 2(4), pp. 40-50
36.
Yenesew A., Twinomuhwezi
H., Kabaru JM., Akala HM., Kiremire BT., Heydenreich M., Peter MG., Eyase FL.,
Waters NC.. Walsh DS. (2009). Antiplasmodial and larvicidal flavonoids from
Derris trifoliata. Bull. Chem. Soc. Ethiop. 23(3), 409-414.
37.
Muiva, LM, Yenesew, A.,
Derese S., Heydenreich M., Peter MG., Akala HM., Eyase L.F, Waters NC.,
Schnabel D., Walsh DS. (2009). Antiplasmodial β-hydroxydihydrochalcone from
seeds and pods of Tephrosia elata. Phytochemistry letters vol 2 no. 3 (2009)
99-102
38.
Midiwo, JO. Omoto, FM.,
Yenesew, A., Akala, HM., Wangui, J., Liyala, P., Wasunna, C., Waters, NC.(2007).
The first 9-hydroxyhomoisoflavanone, and antiplasmodial chalcones, from the
aerial exudates of Polygonum senegalense. ARKIVOC 2007 (ix) 21-27
39.
Abosi A.O., Mbukwa E.,
Majinda R.R.T., Raseroka B.H. * Yenesew A., Midiwo J.O., Akala H., Liyala P. and
Waters N.C. Vangueria infausta root bark: in vivo and in vitro antiplasmodial
activity. BRITISH Journal of Biomedical Science 2006 63 (3), 129-133
40.
Andayi AW., Yenesew A.,
Derese S., Midiwo JO., Gitu PM., Jondiko OJI., Akala H., Liyala P., Wangui J.,
Waters NC., Heydenreich M. Peter MG. Antiplasmodial Flavonoids from Erythrina
sacleuxii. Planta med 2006; 72: 187-189
41.
Yenesew A., Induli, M.,
Derese, S., Midiwo, JO., Heydenreich, M., Peter, MG. Akala, H., Wangui, J.,
Liyala, P., Waters, NC. Anti-plasmodial flavonoids from the stem bark of
Erythrina abyssinica. Phytochemistry 65 (2004) 3029–3032. October 2004,
www.elsevier.com/locate/phytochem.
42.
Mbaisi, A.., Liyala, P.,
Eyase, F., Achilla, R., Akala, H., Wangui, J., Mwangi, J. Osuna, F., Alam, U.,
Smoak, BL., Davis, JM., Kyle, DE., Coldren, RL., Mason, C., Waters, NC. Drug
Susceptibility and Genetic Evaluation of Plasmodium falciparum Isolates Obtained
in Four Distinct Geographical Regions of Kenya. Antimicrobial Agents And
Chemotherapy, Sept. 2004, p. 3598–3601 Vol. 48, No. 9
43.
Yenesew, A., Derese, S.,
Midiwo, JO. Oketch-Rabah, HA. Lisgarten, J. Heydenreich, M., Peter, MG. Akala,
H., Wangui, J., Liyala, P., Waters, NC. Anti-plasmodial Activities and X-ray
Crystal Structures of Rotenoids From Milletia usaramensis Subspecies
Usaramensis, Phytochemistry; 64, 3 (2003) 773-779, July 2003.
44.
Yenesew, A., Derese, S.,
Irungu, B., Midiwo, JO., Waters, NC. Liyala, P. Akala, H., Heydenreich, M.,
Peter, MG. Flavonoids and Isoflavonoids with antiplasmodial activities from the
roots of Erythrina abyssinica; Planta Med, March 2003;69:658-661.
.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What we door: #C0C0C0;">
What we do
|
|
|
Nairobi |
|
 |
|
USAMRD-K Headquarters is located in Nairobi, Kenya on the campus of the Kenya
Medical Research Institute (KEMRI). |
|
|
|
|
|
|
|
The USAMRD-K Department of Emerging Infectious Diseases is based in
Nairobi with numerous satellite collection sites located throughout Kenya,
Tanzania, Uganda and Cameroon executing the Department of Defense Global
Emerging Infections Surveillance and Response System (DoD GEIS).
The USAMRD-K Department of Military to Military Activities and President’s
Emergency Plan for AIDS Relief (PEPFAR) program is based in Nairobi. The focus
of this program encompasses HIV/AIDS prevention and treatment, surveillance for
influenza and other diseases that impact force protection and health readiness
in the Kenyan military and research on medical issues of mutual interest.
|
|
|
|
Kericho |
|
 |
|
The USAMRD-K Kericho Field Station is based in Kericho, Kenya. This
program is primarily funded through the Military HIV Research Program and PEPFAR
with the focus of developing drugs and vaccines for HIV prevention and
treatment.
|
|
|
|
Kisumu |
|

|
|
The USAMRD-K Kisumu Field Station is based in Kisumu, Kenya located in Nyanza
Province along Lake Victoria. There are five clinic and research departments to
include Clinical Trials, Basic Science, Malaria Diagnostics Center (MDC),
Entomology/Vector Biology Unit, and Malaria
Drug Resistance (MDR) Laboratory. The focus of this program is to develop drugs
and vaccines for malaria and other tropical diseases.
|
|
Entomology
|
|
|
The Entomology Program/Vector Biology Unit conducts research on the biology and
ecology of vectors of medical and military important diseases with a focus on
the development of integrated disease surveillance and management strategies.
This department is based on the Kisian KEMRI-campus in western Kenya.
Additionally, the Entomology program has six remote field collection sites
located in Marigat, Kakamega, Busia, West Pokot, Garissa, Wajir, Isiolo, and
Lamu. Future field collection sites will be established in Tanzania, Ethiopia,
and Uganda. The goals of the Entomology program are to develop products, tools,
and methods to mitigate risk and/or prevent vector-borne diseases.
Major research efforts include sand fly surveillance for leishmaniasis in the
Horn of Africa; evaluation of vector control methods e.g. repellent testing;;
arbovirus surveillance; malaria transmission and blocking assays, rodent-borne
viruses’ surveillance (Hantavirus study);; and development of rapid diagnostic
tests for infected vectors.
|
|
|
|
|

Trapped mosquitoes using CDC traps |
|
|
|
|
|
|
|
OVERVIEW |
|
|
|
|
The Entomology Program/Vector Biology Unit conducts research on the biology
and ecology of vectors of military and civilian important diseases with a focus
on the development of integrated disease surveillance and management strategies.
The goals of the Entomology program are to develop products, tools, and methods
to mitigate risk and/or prevent vector-borne diseases.
|
|
|
|
|
|
|
|
|

Kisian Biocontainment level II insectray

|
|
|
|
|
|
|
|
|
The USAMRD-K Entomology insectary is a well equipped Arthropod Containment Level
2 (ACL-2) / BSL-2 facility with an infection suite for maintaining infected
mosquito and sand fly colonies. The insectary is located at the KEMRI Center for
Global Health Research (CGHR) in Kisian near the USAMRD-K Kisumu Field Station.
The insectary maintains two colonies of Anopheles gambiae and one colony of
Anopheles arabiensis mosquitoes that are predominant malaria vectors in a
holoendemic region of Western Kenya. Approximately 720,000 mosquitoes and
500,000 sand flies are reared and maintained annually by 3 full time
technicians.
In the past three years over 2,000,000 mosquitoes and 1,500,000 sand flies have
been produced to support a variety of studies. These include laboratory and
semi-field studies on the evaluation of repellents, insecticides, rodent
pesticide feed-through techniques, malaria transmission and blocking assays as
well as mosquito vector competence studies. The recent study being the malaria
transmission dynamics study (TDS); which one of objectives was to quantify
transmission of Plasmodium falciparum from human population within the study
area to lab-reared An.gambiae after direct feeding (DFA) and membrane feeding
(MFA) assays.

Making paper cups for sandfly sorting

Fixing of Terminator ULV pesticide applicator. ULV means
Ultra-low volume
|
|
|
|
|
The insectary also provides a unique service to the military and the nation. The
USAMRD-K Kisumu Field Station is located in one of the highest P. falciparum
malaria transmission zones in the world and provides a unique opportunity to
study this disease and its natural vectors. Unfortunately, these benefits also
present risks to study participants and challenges in obtaining IRB approvals.
The insectary provides infection-free vectors combined with a new 2000 ft2
semi-field enclosure to conduct behavioral studies or repellent efficacy trials
with decreased risk to study participants and reduced regulatory hurdles.
Finally, the insectary is a core part of a training and education program that
includes both DoD and Kenyan research scientists and students. Approximately 200
Kenyan college students per year rotate through the USAMRD-K labs for two weeks
at a time to gain skills in medical entomology research. It is often through
this pool of students that we hire technicians to work in the labs. From the US
military, insectary rearing operations are part of annual training programs for
selected students from the US Military Academy as well as USUHS Military
Tropical Medicine fellows. |
|
|
|
|
Mission Statement: |
|
Conduct research and surveillance in support of the development of integrated
pest management strategies against arthropod-borne pathogens. |
|
|
Vision Statement: |
|
To research and develop novel disease control strategies and test products that
help discover, mitigate and/ or prevent vector borne diseases in Kenya and
beyond. |
|
|
Publications |
|
Download
the PDF |
|
1. Elizabeth Wanja, Zahra Parker, Tobin Rowland, Michael J.
Turell, Jeffrey W. Clark, Kirti Davi, Sonia Davi and Rosemary Sang, Field
Evaluation of a Wicking Assay for the Rapid Detection of Rift Valley Fever Viral
Antigens in Mosquitoes, Journal of the American Mosquito Control Association,
27(4):370-375, 2011
2. Clark J.W, Kioko E, Odemba
N, Ngere F , Kamanza J, Oyugi E, Kerich G, Kimbita E, and Bast J.D. First Report
of the Visceral Leishmaniasis Vector Phlebotomus martini (Diptera: Psychodidae)
in Tanzania. J. Med. Entomol. 50(1): 212-216 (2013).
3. Sherwood V, Kioko E , Kasili S, Ngumbi P
Hollingdale MR. Field trial of five Repellent formulations Against Mosquitoes in
Ahero, Kenya. The United States Army Medical Department Journal.July-Sep
2009.60-5.
4. Kasili S, Odemba N, Ngere F, Kioko E, Kamanza J,
Muema A and Kutima HL Entomological assessment of the potential for malaria
transmission in Kibera slum of Nairobi, Kenya. J Vector Borne Dis 46, December
2009, pp. 273–279.
5. Kasili S, Ngumbi PM, Koka H, Ngere F, Kioko E,
Odemba N and Kutima HL Comparative performance of light trap types, lunar
influence and sandfly abundance in Baringo district, Kenya. J Vector Borne Dis
47 June 2010,pp 108-112.
6. T.M. Mascari,R.W. Stout,J.W. Clark,S.W. Gordon,
J.D. Bast L.D. Foil. Insecticide-treated rodent baits for sand fly control.
Pesticide Biochemistry and Physiology 106 (2013) 113–117
7. Seth C. Britch, Kenneth J. Linthicum, Todd W.
Walker, Muhammad Farooq, Scott W. Gordon, Jeffrey W. Clark, Francis Ngere,
Daniel Ngonga, and Clifford Chepchieng. Evaluation of ULV Applications Against
Old World Sand Fly (Diptera: Psychodidae) Species in Equatorial Kenya. Journal
of Medical Entomology, 48(6): 1145–1159. 2011.
8. Sancto Yalwala, Jeffrey Clark, David Oullo, Daniel
Ngonga, David Abuom, Elizabeth Wanja and Joshua Bast. Comparative efficacy of
existing surveillance tools for Aedes aegypti in Western Kenya. Vector Ecology
40 (2): 301-307. 2015.
9.
Santos Yalwala, Jason W. Kollars, Geoffrey Kasembeli,
Chris Barasa, Charles Senessie, Peggy G. Kollars, Thomas M. Kollars Jr.
Preliminary Report on the Reduction of Adult Mosquitoes in Housing Compounds in
Western Kenya Using the ProVector Flower and Entobac Bait Pads Containing
Bacillus thuringiensis israelensis With Honey Bait. J Med Entomology 2016 Jun 9.
Epub 2016 Jun 9.
|
|
|
|
|
|
|
|
|
|
Malaria Diagnostics Center
|
|
|
|
|
|
|
Malaria Diagnostics Centre (MDC), a department of the KEMRI/USAMRD-K located in
Kisumu, Kenya is the largest malaria diagnostic center in sub-Saharan Africa.
The MDC was established in 2004 to conduct malaria diagnostic training. The
center leads global effort in training to improve malaria diagnostics capacity
and quality at laboratories in Kenya, across Africa, Europe, Asia, South
America, and the United States.
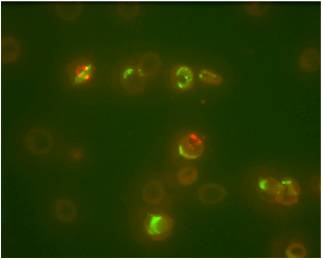
Malaria microscopy remains the gold standard for malaria diagnosis in clinical
trials, new diagnostic methodology evaluation and clinical care. Due to its
location in a highly malaria endemic region of Kenya, MDC has the advantage of
having a continuous supply of samples for human malaria parasites through its
Blood Collection Protocol (BCP). These samples are used for preparation of blood
films that are stored in our slide bank; these slides are used for training and
testing laboratory technicians, developing and managing malaria quality
assurance programs, they are also available to other institutions upon request.
The samples collected are also used for testing of novel diagnostic devices and
assays.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
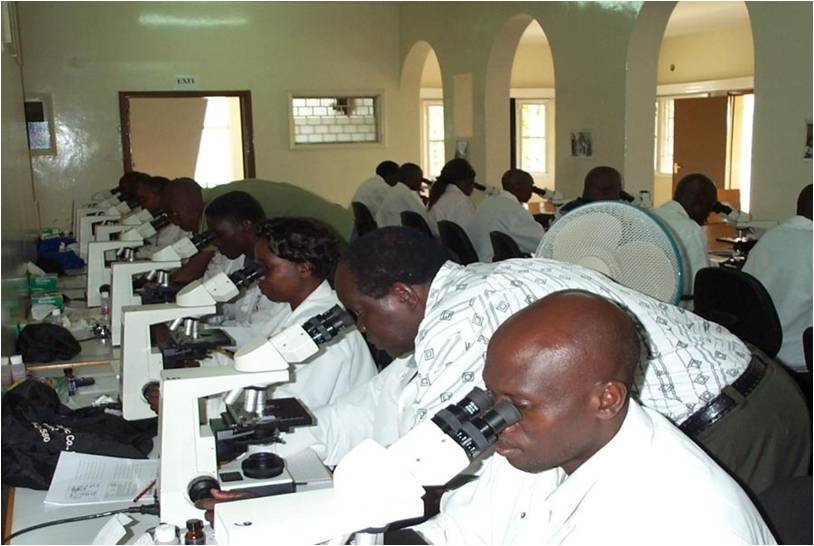
MDC has designed standardized skill based training and
assessment programs in a bid to improve competency and strengthen diagnosis of
malaria. The trainings consists of didactic and practical instructions on
– Life cycle of malaria
– Clinical presentation of malaria
– Parasite detection, counting, Plasmodium species
identification
– Blood film preparation and staining
– Identification of artifacts and pseudo-parasites
– Techniques for detecting mixed infections and low
density infections
– Standard operating procedure development
– Laboratory quality assurance and quality control
– Rapid diagnostic testing technique
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All our facilitators at the centre are WHO certified malaria microscopists thus
ensuring quality training. MDC has trained over 2500 laboratory technicians from
Kenya and other countries all over the world. We have also trained military
personnel from both East and West Africa under the African Malaria Task force
initiative. We have also supported the established the set up of other MDC
centers in Nigeria, Tanzania and Ghana. The training is open to laboratory
technicians, technologists, researchers/scientists or tutors from medical
training colleges & universities with a minimum of a certificate or diploma in
medical laboratory or a related field. Below are some of the trainings that MDC
offers:-
1. Two weeks basic malaria microscopy training
2. One week microscopy refresher training
3. Two weeks malaria EQA training
4. One week tailor-made malaria microscopy training (based on needs of an
organization or the sponsor)
5. Three day RDT training
|
|
|
|
|
|
|
|
|
|
 |
 |
|
|
|
|
|
|
|
|
|
Malaria training resources
|
|
|
|
|
• 35 binocular microscopes
• 15 highly proficient trainers & support staff
• 10-head training microscope with digital camera
• Digital multimedia presentation capabilities
• Student lap-tops and monitors
• 2 clinical trial sites at Kondele and Kombewa
• Validated malaria reference slides for training, proficiency testing and
certification
• Photographic malaria parasite Images
• On-site kitchen provides meals |
|
|
|
|
|
|
|
|
|
Malaria EQA Support
|
|
|
|
|
MDC also offers malaria EQA services to various clinical trials such as the
Malaria Clinical Trials Alliance (MCTA), European Developing Countries Clinical
Trial Partnership (EDCTP), AIDS Clinical Trial Group (ACTG), Sanofi Aventis just
to mention a few. We also offer support to the Kenyan Ministry of Health,
National Malaria Control Program and we have been involved in offering our
malaria microscopy service in the three Kenya Malaria Indicator Surveys carried
out in the country |
|
|
|
|
|
Publications
Download the PDF |
|
|
|
|
1. Field evaluation of diagnostic performance of malaria rapid diagnostic tests
in western Kenya Malar J 15:456
2. Establishing a Malaria Diagnostics Centre of Excellence in Kisumu Kenya -
Malar J.6:79
3. Pilot assessment of the sensitivity of the thin film - Malar J.7:22
4. Systematic Comparison of two methods to measure parasite density from malaria
blood smears Parasitol Res 99:500-506
5. Misclassification of Plasmodium infections by conventional microscopy and the
impact of remedial training on the proficiency of
laboratory technicians proficiency in species identification – Malar J.12:113 |
|
|
|
|
|
|
|
Basic Science Lab
|
|
Overview:
|
|
|
|
The USAMRD-K Basic Science laboratory is a research laboratory that performs
multi-disciplinary molecular and Immunology research in malaria and other
infectious diseases, including disease surveillance, diagnostic evaluations and
development and vaccine efficacy evaluations. It is comprised of 32 highly
trained laboratory and field staff and has the capacity to run assays using
state of the art techniques. |
|
|
|
|
|
|
Mission Areas:
|
|
|
|
Supports USAMRU-D’s broader mission of health security by:
– Providing disease surveillance and assisting in outbreak investigations for infectious
diseases of military and global health relevance
– Supporting development of diagnostic platforms for diseases of Africa and the
world
– Providing basic science support to vaccines and drug trials evaluations
– Building capacity for young Kenyans in various areas including molecular
biology and immunology
|
|
|
|
|
|
|
Vision statement:
|
|
|
|
To use scientific mandate and accompanying resources to:
1. Improve research capability of local scientist
2. Improve knowledge on disease distribution in the country
3. Become a leading standard bearer of excellent medical research, disease
surveillance, diagnosis, management and training in medical research in Kenya
and beyond.
|
|
|
|
|
|
|
Our resources:
|
|
|
|
– 32 well trained Lab and field staff
– qPCR and conventional PCR platforms
– 8 color flow-cytometer
– Malaria parasite culture capability
– MAGPIX platform for multiplexing pathogen ID
– MiSeQ platform for whole genome sequencing to allow pathogen characterization
and discovery
– Well developed infrastructure for basic science research
|
|
|
|
|
Our Partners |
|
|
|
|
• U.S. Government
– US DOD GEIS – USAMRIID
– MIDRP – US CDC
• Kenya Government
– Kenya Medical Research Institute
– MOH
– Department of Veterinary Services
– Academia
– International and NGO |
• PATH
– BioFire
– SMEs
– MBIO Diagnostic, Boulder CO
– SIGHT Diagnostics, Israel
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Publications |
Download the PDF |
|
|
|
1) Masakhwe C, Ochanda H, Nyakoe N, Ochiel D, Waitumbi J (2016) Frequency of
Epstein - Barr Virus in Patients Presenting with Acute Febrile Illness in Kenya.
PLoS ONE 11(5): e0155308. doi:10.1371/journal.pone.0155308
2) Kimita G, Mutai B, Nyanjom SG, Wamunyokoli F, Waitumbi J (2016) Phylogenetic
Variants of Rickettsia africae, and Incidental Identification of "Candidatus
Rickettsia Moyalensis" in Kenya. PLoS Negl Trop Dis 10(7): e0004788.
doi:10.1371/journal.pntd.0004788
3) Miller RH, Obuya CO, Wanja EW, Ogutu B, Waitumbi J, Luckhart S, et al. (2015) Characterization of
Plasmodium ovale curtisi and P. ovale wallikeri in Western Kenya Utilizing a
Novel Species-specific Real-time PCR Assay. PLoS Negl Trop Dis 9(1): e0003469.
doi:10.1371/journal.pntd.0003469
4) Jacqueline W. Thiga, Beth K. Mutai, Wurapa K. Eyako, Zipporah Ng’ang’a, Ju
Jiang, Allen L. Richards, John N. Waitumbi. High Seroprevalence of Antibodies
against Spotted Fever and Scrub Typhus Bacteria in Patients with Febrile
Illness, Kenya Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 21, No. 4,
April 2015
5) Martin Maina Wahome, Josphat Nyandieka Nyataya, Hosea Miima Akala, George
Odhiambo Awinda, Beth Kinya Mutai, Rebecca Waihenya, Edwin Kamau, Sabah Ahmed
Omar, John Njenga Waitumbi. Chloroquine Tolerance in 3D7 Strain of P. falciparum
was Associated with Change in Allelic Structure and not Pfcrt and Pfmdr1
Transporter Genes nor DNA Methylation. American Journal of Biology and Life
Sciences. Vol. 2, No. 5, 2014, pp. 100-107
6) Korir JC, Nyakoe NK, Awinda G, Waitumbi JN (2014) Complement Activation by
Merozoite Antigens of Plasmodium falciparum. PLoS ONE 9(8):
e105093.doi:10.1371/journal.pone.0105093
7) Mutai BK, Wainaina JM, Magiri CG, Nganga JK, Ithondeka PM, Njagi ON, Jiang J,
Richards AL, Waitumbi JN. Zoonotic surveillance for rickettsiae in domestic
animals in Kenya. Vector Borne Zoonotic Dis. 2013 Jun;13(6):360-6. doi:
10.1089/vbz.2012.0977. Epub 2013 Mar 11.
8) Nash Michael A, Waitumbi John N, Hoffman Allan S, Yager Paul, Stayton Patrick
S. 2012. "Multiplexed enrichment and detection of malarial biomarkers using a
stimuli-responsive iron oxide and gold nanoparticle reagent system." ACS nano 6
(8): 6776-85. doi:10.1021/nn3015008.
9) Korir Jackson C, Magambo Japhet K, Mwatha Joseph K, Waitumbi John N. 2012.
"B-cell activity in children with malaria." Malaria journal 11: 66.
doi:10.1186/1475-2875-11-66.
10) Kamau Edwin, Tolbert Ladonna S, Kortepeter Luke, Pratt Michael, Nyakoe
Nancy, Muringo Linda, Ogutu Bernard, et al. 2011. "Development of a highly
sensitive genus-specific quantitative reverse transcriptase real-time PCR assay
for detection and quantitation of plasmodium by amplifying RNA and DNA of the
18S rRNA genes." Journal of clinical microbiology 49 (8): 2946-53.
doi:10.1128/JCM.00276-11.
11) Waitumbi John N, Gerlach Jay, Afonina Irina, Anyona Samuel B, Koros Joseph
N, Siangla Joram, Ankoudinova Irina, et al. 2011. "Malaria prevalence defined by
microscopy, antigen detection, DNA amplification and total nucleic acid
amplification in a malaria-endemic region during the peak malaria transmission
season." Tropical medicine & international health : TM & IH 16 (7): 786-93.
doi:10.1111/j.1365-3156.2011.02773.x.
12) Carter Nick, Pamba Allan, Duparc Stephan, Waitumbi John N. 2011. "Frequency
of glucose-6-phosphate dehydrogenase deficiency in malaria patients from six
African countries enrolled in two randomized anti-malarial clinical trials."
Malaria journal 10: 241. doi:10.1186/1475-2875-10-241.
13) Blaylock JM, Maranich A, Bauer K, Nyakoe N, Waitumbi J, Martinez LJ, Lynch
J. The seroprevalence and seroincidence of dengue virus infection in western
Kenya. Travel Med Infect Dis. 2011 Sep;9(5):246-8. doi:
10.1016/j.tmaid.2011.06.005. Epub 2011 Jul 20.
14) Waitumbi John N, Kuypers Jane, Anyona Samuel B, Koros Joseph N, Polhemus
Mark E, Gerlach Jay, Steele Matthew, et al. 2010.
"Outpatient upper respiratory tract viral infections in children with malaria
symptoms in Western Kenya." The American journal of tropical medicine and
hygiene 83 (5): 1010-3. doi:10.4269/ajtmh.2010.10-0174.
15) Woodring Joseph V, Ogutu Bernhards, Schnabel David, Waitumbi John N, Olsen
Cara H, Walsh Douglas S, Heppner D Gray, et al. 2010. "Evaluation of recurrent
parasitemia after artemether-lumefantrine treatment for uncomplicated malaria in
children in western Kenya." The American journal of tropical medicine and
hygiene 83 (3): 458-64. doi:10.4269/ajtmh.2010.09-0403.
16) Beth K Mutai, John N Waitumbi. Apoptosis stalks Plasmodium falciparum
maintained in continuous culture condition Malaria Journal 2010, 9(Suppl 3):S6
17) Robert N Maina, Douglas Walsh, Charla Gaddy, Gordon Hongo, John Waitumbi,
Lucas Otieno, David Jones and Bernhards R Ogutu. Impact of Plasmodium falciparum
infection on haematological parameters in children living in Western Kenya
Malaria Journal20109(Suppl 3):S4
18) Walsh Douglas S, Eyase Fredrick, Onyango David, Odindo Alfred, Otieno
Walter, Waitumbi John N, Bulimo Wallace D, et al. 2009. "Short report: Clinical
and molecular evidence for a case of Buruli ulcer (Mycobacterium ulcerans
infection) in Kenya." The American journal of tropical medicine and hygiene 81
(6): 1110-3. doi:10.4269/ajtmh.2009.09-0313.
19) Nyakoe Nancy K, Taylor Ronald P, Makumi Joseph N, Waitumbi John N. 2009.
"Complement consumption in children with Plasmodium falciparum malaria." Malaria
journal 8: 7. doi:10.1186/1475-2875-8-7.
20) Ogutu Bernhards R, Apollo Odika J, McKinney Denise, Okoth Willis, Siangla
Joram, Dubovsky Filip, Tucker Kathryn, et al. 2009. "Blood stage malaria vaccine
eliciting high antigen-specific antibody concentrations confers no protection to
young children in Western Kenya." PloS one 4 (3): e4708.
doi:10.1371/journal.pone.0004708.
21) Waitumbi John N, Anyona Samuel B, Hunja Carol W, Kifude Carolyne M, Polhemus
Mark E, Walsh Douglas S, Ockenhouse Chris F, et al. 2009. "Impact of
RTS,S/AS02(A) and RTS,S/AS01(B) on genotypes of P. falciparum in adults
participating in a malaria vaccine clinical trial." PloS one 4 (11): e7849.
doi:10.1371/journal.pone.0007849.
22) Polhemus Mark E, Remich Shon A, Ogutu Bernhards R, Waitumbi John N, Otieno
Lucas, Apollo Stella, Cummings James F, et al. 2009. "Evaluation of RTS,S/AS02A
and RTS,S/AS01B in adults in a high malaria transmission area." PloS one 4 (7):
e6465. doi:10.1371/journal.pone.0006465.
23) Kifude Carolyne M, Rajasekariah Halli G, Sullivan David J, Stewart V Ann,
Angov Evelina, Martin Samuel K, Diggs Carter L, et al. 2008. "Enzyme-linked
immunosorbent assay for detection of Plasmodium falciparum histidine-rich
protein 2 in blood, plasma, and serum." Clinical and vaccine immunology: CVI 15
(6): 1012-8. doi:10.1128/CVI.00385-07.
24) Pawluczkowycz Andrew W, Lindorfer Margaret A, Waitumbi John N, Taylor Ronald
P. 2007. "Hematin promotes complement alternative pathway-mediated deposition of
C3 activation fragments on human erythrocytes: potential implications for the
pathogenesis of anemia in malaria." Journal of immunology (Baltimore, Md. :
1950) 179 (8): 5543-52.
25) Kifude Carolyne M, Polhemus Mark E, Heppner D Gray, Withers Mark R, Ogutu
Bernhards R, Waitumbi John N. 2007. "Hb Kenya among Luo adults and young
children in malaria holoendemic Western Kenya: screened by high performance
liquid chromatography and confirmed by polymerase chain reaction." Hemoglobin 31
(4): 401-8. doi:10.1080/03630260701587638.
26) Withers Mark R, McKinney Denise, Ogutu Bernhards R, Waitumbi John N, Milman
Jessica B, Apollo Odika J, Allen Otieno G, et al. 2006. "Safety and
reactogenicity of an MSP-1 malaria vaccine candidate: a randomized phase Ib
dose-escalation trial in Kenyan children." PLoS clinical trials 1 (7): e32.
doi:10.1371/journal.pctr.0010032.
27) Anyona Samuel B, Schrier Stanley L, Gichuki Charity W, Waitumbi John N.
2006. "Pitting of malaria parasites and spherocyte formation." Malaria journal
5: 64. doi:10.1186/1475-2875-5-64.
28) Craig Maria L, Waitumbi John N, Taylor Ronald P. 2005. "Processing of
C3b-opsonized immune complexes bound to non-complement receptor 1 (CR1) sites on
red cells: phagocytosis, transfer, and associations with CR1." Journal of
immunology (Baltimore, Md. : 1950) 174 (5): 3059-66.
29) Waitumbi John N, Donvito Béatrice, Kisserli Aymric, Cohen Jacques H M,
Stoute José A. 2004. "Age-related changes in red blood cell complement
regulatory proteins and susceptibility to severe malaria." The Journal of
infectious diseases 190 (6): 1183-91. doi:10.1086/423140.
30) Ohas Eunita A, Adams John H, Waitumbi John N, Orago Alloys S S, Barbosa
Arnoldo, Lanar David E, Stoute José A, et al. 2004. "Measurement of antibody
levels against region II of the erythrocyte-binding antigen 175 of Plasmodium
falciparum in an area of malaria holoendemicity in western Kenya." Infection and
immunity 72 (2): 735-41.
31) Stoute José A, Odindo Alfred O, Owuor Boaz O, Mibei Erick K, Opollo Malachi
O, Waitumbi John N. 2003. "Loss of red blood cell-complement regulatory proteins
and increased levels of circulating immune complexes are associated with severe
malarial anemia." The Journal of infectious diseases 187 (3): 522-5.
doi:10.1086/367712.
|
|

USAMRD-K DEID
|
|
|
|
|
|
|
USAMRD-K DEID formerly known as USAMRD-K GEIS is the Kenyan arm of the United
States DoD Global Emerging Infectious Surveillance and Response System
(DoD-GEIS) a core component of the Armed Forces Health Surveillance Center
(AFHSC). Being part of the global DoD GEIS partnership, USAMRD-K DEID, promotes
and facilitates national and international preparedness for emerging infections
to protect the health of the public at large and US-DoD personnel. USAMRD-K DEID
continues to promote, expand and execute its strategic goals of surveillance and
detection; response and readiness; integration and innovation and cooperation
and capacity building. |
|
|
|
|
This is an acronym denoting United States Army Medical Research Directorate
USAMRD-K carries out medical research by developing and testing improved means of predicting, detecting, prevention and treating disease-threats important to the US Army.
USAMRD-K also conducts surveillance, training and response activities related to emerging infectious disease-threats.
What we do
USAMRD-K has it Kenyan Headquarters situated within KEMRI HQs off Mbagathi Road
in Nairobi, the capital City of Kenya. It has two major field sites namely
Kisumu and Kericho field stations. Kisumu Field station is located in Kondele
area along Kisumu – Kakamega Road, with its Centre for Clinical Research
situated in Kombewa off Bondo - Usenge Road, opposite the Kombewa Sub-County
Hospital. Kericho Field Station is in USHMA plaza along Temple Road, Kericho
town
Contact usssssssssssssssss="style4">Contact ussssssssssssssss
|
|
|
News and Events |
-
 -
Respiratory Infections Influenza viruses
continue to be very unpredictable, with the recent...
|
|
Latest Publications NEW
Misclassification of Plasmodium infections by conventional microscopy and the
impact of remedial training on the proficiency of...
View the Publication Certified Mosquito Identification Specialists
NEW
USAMRD-K congraulates Dunstone Beti and James Mutisya on their declaration as
Certified Mosquito Identification Specialists.
Latest Publications NEW Mosquito-borne
arbovirus surveillance at selected sites in diverse ecological zones of Kenya,
2007 – 2012. View the
Publication Latest
Publications NEW The Role of Pfmdr1 and Pfcrt in Changing
Chloroquine, Amodiaquine, Mefloquine and Lumefantrine Susceptibility in
Western-Kenya...
View the Publication Latest Publications NEW Detection
of Avian Influenza Viruses in Wild Waterbirds in the Rift Valley of Kenya Using
Fecal Sampling, Vector-borne and Zoonotic Diseases.
View the
Publication
|
|
|
-
 -
Malaria Drug Resistance Kenya, an epicenter of Malaria drug resistance
emergency in Africa...
|
|
|
|
|
-
-
Febrile
& Vector Borne Illnessess Influenza viruses continue to be very
unpredictable, with the recent...
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Global Emerging Infections Surveillance and Response System (GEIS) Division
at the AFHSC contributes to the protection of all Department of Defense (DoD)
healthcare beneficiaries and the global community through an integrated
worldwide emerging infectious disease surveillance system. GEIS was created in
1997 in response to Presidential Decision Directive NSTC-7 to provide a
mechanism within the DoD to centralize coordination of surveillance efforts
conducted through DoD overseas medical research and development laboratories.
Efforts ultimately support and strengthen surveillance among deployed US
military personnel and aid in diagnosis and treatment at military treatment
facilities. Additionally, all host country partner activities are directed
toward improvement of each country's diagnostic and reporting requirements in
accordance with World Health Organization's International Health Regulations
(2005) core capacities.
The integrated emerging infectious disease system supported by GEIS is guided by
four strategic goals:
• Conduct surveillance and outbreak response activities,
• Expand surveillance and epidemiology training and capacity building within the
US military and in partner nations,
• Support research, innovation and integration initiatives that emphasize an
eventual product that will enhance force health protection such as drug and
diagnostic tool development, and
• Assessment and communication of value added by the network.
Surveillance priorities are:
• Respiratory infections
• Febrile and vector infections (including malaria)
• Gastrointestinal infections • Antimicrobial resistant organisms
• Sexually transmitted infections
• Capacity Building and biosurveillance systems
Through generous funding from AFHSC-GEIS, USAMRD-K GEIS, now known as USAMRD-K
DEID, was started in Kenya through an existing cooperative agreement with KEMRI
in 1998, and expanded to Uganda, Tanzania and Cameroon in subsequent years. This
was necessitated by the inadequate surveillance and outbreak response capacities
in most Sub Saharan countries where most disease outbreaks go undetected.
USAMRD-K DEID currently undertakes research and surveillance in the following
areas:
• Influenza (Human, Avian and Swine)
• Arbovirology • Viral Hemorrhagic Fever
• Acute Febrile Illnesses, • Leishmaniasis,
• Enteric Diseases
• Sexually Transmitted Diseases
• Rodent Borne Viruses
• Health Demographics
• Malaria Drug Dusceptibility
These activities are spread out across facilities in Africa as follows:
|
Kenya |
|
Uganda |
|
• The National Influenza
Center located at the Center for Public Health Research in KEMRI, Nairobi
• The Arbovirology/Viral Hemorrhagic Fever Laboratory
located at the Center for Virus Research Research in KEMRI, Nairobi
• The National Malaria Drug Resistance Surveillance
Laboratories in Kisumu, Western Kenya
• The Rodent Borne Virus Project in Kisumu, Western
Kenya
• The Kisumu West Health and Demographic Surveillance
System (KWHDSS) in Kisumu West District
• The Microbiology Hub in Kericho for Enterics
Surveillance in South Western Kenya
• The Gonorrhea Drug Susceptibility Surveillance
Laboratories in KEMRI, Nairobi
• The East Africa/Horn of Africa Leishmaniasis (HOA)
Surveillance Project in Kisumu, Western Kenya
• The Acute Febrile Illness Surveillance Project
Laboratories in Kisumu, Western Kenya
• The Domestic Avian Influenza Surveillance Laboratories
in Kisumu, Western Kenya
|
|
• The Makerere University Walter Reed Project (MUWRP) for
Influenza Surveillance Laboratories located at the Uganda Virus Research
Institute (UVRI) in Entebbe and Makerere University College of Veterinary
Medicine in Kampala, Uganda.
|
|
Tanzania |
|
• The Tanzania People’s Defense Force (TPDF)
USAMRD-K-DEID program, Lugalo Military Hospital in Dar es Salam, Tanzania
|
|
Cameroon |
• The Global Viral Forecasting (GVF) for Influenza
Surveillance Laboratory located at the Centre de Recherche de Santé des Armées
or the Military Health Research Center, (CRESAR) in Yaounde, Cameroon
• The laboratory for Emerging Infectious Diseases (LEID)
located at the University of Buea (UoB) in Buea South West region, Cameroon
|
|
|
|
|
|
|
|
USAMRD-K DEID is now making a difference in Influenza surveillance and detection
capabilities. Additionally, researchers at USAMRD-K DEID play a vital role in
helping to predict and prevent zoonotic diseases which according to the World
Health Organization (WHO) make up more than 60% of all human infectious diseases
and more than 70% of all emerging infectious diseases. USAMRD-K DEID has
rigorous bio-safety/bio-security standards compliant with the internationally
accepted standards of the WHO. USAMRD-K DEID is also involved in extensive
capacity building in all countries of operation through training to improve the
host countries public health infrastructure for disease surveillance and
research. Overall, our robust surveillance network plays a critical role in
outbreak prediction, mitigation and response. |
|
|
|
|
|
Researchers at USAMRD-K DEID focus on several areas of research
pertaining to
the human-animal interface that could have a profound
impact on protecting human
health.
|
THE ARBOVIROLOGY/VIRAL HEMORRHAGIC FEVER (VHF) LABORATORY |
|
|
|
|
|
The laboratory housed in the Centre for Virus Research, Kenya Medical Research
Institute (KEMRI) is headed by Dr. Rosemary Sang (MSc. Medical Virology, PhD
Medical Entomology) and managed by Lillian Musila (BSc. Microbiology, PhD
Molecular Parasitology). The laboratory has the capacity to perform: ELISAs,
virus cultures in various cell lines, animal inoculations, plaque assays,
immuno-fluorescence assays, conventional and real-time PCR, vector competence
tests, arthropod vector sampling and identification, mosquito rearing and
outbreak response. The laboratory is mandated to provide support for public
health action and response in respect to arbovirus and hemorrhagic fever virus
emergencies. We conduct surveillance to monitor arbovirus infections and/or
transmission in diverse human and vector populations at sites in Kenya. These
are selected on the basis of past documented outbreaks and incidence of disease
and other vulnerability factors towards understanding their epidemiology and
developing diagnostics and control strategies.
|
|
|
|
|
-

Trapped mosquitoes being loaded to a truck for transportation to the laboratory
for analysis.
-
 , ,
-
A trap with mosquitoes before disassembly.
-

-
VHF staff at the USAMRD-K-DEID HQ.
|
In addition, we participate in outbreak investigation and response supporting
activities both in Kenya and the East African region. We perform vector
competency studies to evaluate the vector efficiency of mosquito species found
harboring arboviruses. We act on requests from the Kenyan Ministry of Public
Health and Sanitation and the WHO being a member of the WHO Global Outbreak
Alert and Response Network (GOARN) mandated to investigate or respond to
outbreaks of arboviruses.
The laboratory supports research programs focusing on arbovirus epidemiology,
diagnostics and disease control. The ongoing activities in the laboratory are
supported largely by USAMRU – Kenya. The lab participates in the DEID-funded
Acute Febrile Project to detect arboviral causes of undiagnosed febrile
illnesses and runs a DEID funded arbovirus surveillance program for monitoring
the circulation of arboviruses in vector populationsk across Kenya. Other
laboratory support comes from the Centers for Disease Control and Prevention
(CDC), Google, Consortium for National Health Research (CNHR) and the United
States department of Agriculture (USDA). The lab partners in a
multi-organizational Google.org funded project entitled “An integrated response
system for emerging infectious diseases in East Africa” working on arboviruses.
We are also developing diagnostic reagents for arboviral diseases through a
Consortium for National Health Research -Kenya funded project.
We are currently facilitating the following MSC and PhD projects:
Seroprervalence of Crimean Congo Hemorrhagic Fever and West Nile fever among
residents of Ijara and Garissa Districts; Assessment of diversity of Ndumu virus
strains isolated from mosquitoes from various regions in Kenya; Development of
Replenishable, Cost Effective and Stable ELISA Reagents for the detection of
Chikungunya Virus Infection. We also support the DEID student attachment program
by training on average 8 college/university students per month on laboratory
techniques on a rotation basis, we also host longer-term attachment students and
volunteers. The laboratory currently has a work force of 15 people including
researchers, technicians, interns and graduate students.
|
|
|
Partners: |
|
|
|
|
|
• Jomo Kenyatta University of Agriculture and Technology
(JKUAT)
• University of Nairobi (UON) • The International Centre
of Insect Physiology and Ecology (ICIPE) • Ministry of Public Health and
Sanitation (MoPHS)
|
|
• Department of Veterinary Services
• Kenya Wildlife Service (KWS)
• International Centre for Livestock Research (ILRI)
• United States Army Medical Research Institute for Infectious Diseases (USAMRIID) |
|
• University of Texas Medical Branch (UTMB)
• Centers for Disease Control and Prevention (CDC)
• United States Department of Agriculture (USDA)
• World Health Organization (WHO)
|
|
|
|
|
|
|
|
|
|
|
THE INVITRO LABORATORY KISUMU |
|
-
 -
Hosea Akala uses the relative flouresence counts to
depict per drug 50% Inhition concentration (IC50), a measure of drug efficacy
in-vitro.
|
The Malaria parasite culture and drug susceptibility testing laboratory
receives malaria samples from across Kenya, conducts immediate ex vivo
sensitivity (near-by sites) and in vitro (distant sites) sensitivity testing
against a panel of 11 antimalarials namely Chloroquine, Mefloquine, Quinine,
Artemisinin, Amodiaquine, Doxycycline, Artemether, Lumefantrine, Primaquine,
Tafenoquine, Atovaquone.
|
|
|
|
|
|
THE NATIONAL INFLUENZA CENTER |
|
|
|
|
|
|
DEID SUPPORTS PANDEMIC INFLUENZA OUTBREAK RESPONSE IN KENYA AND EAST AFRICA |
|
|
|
|
|
-
 -
The National Influenza team at the
center for public health research, Nairobi.
|
|
In response to the 2009 pandemic influenza A H1N1 outbreak, the Kenya Ministry
of Public Health and Sanitation began implementing its influenza pandemic
preparedness plans in mid May. USAMRD-K DEID officials were consulted on
preparedness, diagnostic, and public outreach planning and implementation
throughout this time period. On June 29 2009, the first case of pandemic
influenza A H1N1 was jointly confirmed in Kenya by the CDC-Kenya and the
USAMRD-K DEID influenza program. Together with ministry officials, the WHO, and
CDC-Kenya personnel, the DEID Coordinator at USAMRD-K, and the program
virologist were co-opted in the planning teams that drew up case definitions,
hospital response, communications, laboratory testing algorithms and other
preparedness and response issues..
Within three months of its introduction into Kenya, pandemic influenza A (H1N1)
virus spread to many parts of the country. In the first three months of the
pandemic outbreak, 1439 samples were sent to the NIC from diverse parts of the
country for diagnostic testing for the presence of the novel 2009 pandemic
influenza A H1N1. Out of these, 233 samples (16%) tested positive for the novel
2009 pandemic influenza A H1N1 strain. |
|
-
 -
Cases in Kenya 2009
|
|
Ninety nine (99) samples from suspected pandemic influenza A H1N1 cases were
sent from the Republic of Seychelles to the Kenyan NIC between May and 10th
October 2009. Close to one half (46%) of these specimens tested positive for
influenza. Among those cases that tested positive for influenza, a majority
(76%) were pandemic influenza A H1N1. Out of the 10 samples received from the
Garowe Hospital in Somalia, 2 tested positive for Pandemic H1N1 virus and 4
tested positive for seasonal influenza A.
By leveraging the capacity and networks built in support of human influenza
sentinel surveillance, DEID supported diagnosis and response to this pandemic in
the region in a timely manner and in line with its global mandate and
objectives. |
 |
|
|
|
|
KENYA STUDENTS INTERNSHIP PROGRAM
|
|
|
A critical part of our capacity building mandate, the DEID attachment program
was initiated in 2002. The program provides laboratory placement, practicum,
internship and other forms of professional, industrial or vocational experience.
The program is designed to provide undergraduates, diploma students and
volunteers with educational training and research experiences to strengthen
their knowledge and skills and deepen their commitment to pursue careers in
medical research. Most importantly it is a way for USAMRD-K DEID to promote the
transfer of scientific knowledge and technology to host country nationals. While
on placement, students are also trained on occupational health & safety, quality
assurance and control and privacy legislation requirements. Student progress is
systematically monitored.
Since December 2006 a total of 75 interns have passed through the program. The
majority of our trainees successfully completed their rotations and are now
gainfully employed or in postgraduate studies. The quality of the program can be
attested by the high number of applications, which averages 180 annually. Our
ultimate vision is to open the program to DEID partner countries and eventually
turn it into a Tropical Medicine training program for students worldwide.
|
|
|
|
|
|
SPECIAL FEATURE: |
Expanding Acute Febrile Illness (AFI) Surveillance to the Somali Basin |
|
|
|
|
|
|
|
Dr. Dahaba Ali says she became a doctor, as she wanted to help her people; the
predominantly ethnic Somalis inhabiting the 126,902 km² North Eastern Province
(NEP). The region spans the entire length of the Somalia border (Fig. 6), with a
1999 population projection showing it to be home to approximately 1.3 million
people. The 2009 census put the figure at 2.3 million.
NEP falls in an arid zone that experiences prolonged droughts often followed by
devastating floods. Apart from river Tana, most other rivers here are
characterized by dry riverbeds. With little possibility for irrigation-based
development, nomadism is the main economic activity. The pastoralists rely on
well water; patchy pasturage necessitating periodical movement. This pastoralism
is based around the Arabian camel, which is well adapted to hot, dry habitats.
Dahaba, quite possibly the only female of the 26 medical doctors in the whole
province is the medical superintendent at Iftin Sub-District Hospital, AFI’s
first site in NEP where surveillance commenced in February 2010. NEP is plagued
by high poverty and illiteracy rates. The province lags behind the rest of the
country in development.
Indeed, NEP has the least developed infrastructure in the country, “we did not
get a good deal- like in roads, there is no road from here (Garissa) to Nairobi,
to Mandera it’s even worse” explains Dahaba, “staff posted between districts
cannot manage to work efficiently as they have no means to get there.”
This underdevelopment is also mirrored in NEP’s health delivery system. Kenya’s
pyramidal public health sector delivers through a referral system, which
requires patients to start at the base, the dispensaries, working their way up
to the hospitals only on referral. Resource scarcity towards the base of the
pyramid however greatly affects health care delivery; the focus on
curative/hospital care invariably centered in urban areas denies distribution of
resources to the more rural based health centers and dispensaries, accessible to
Kenya’s 80% rural population, this is a major problem in NEP where most of the
population is rural poor.
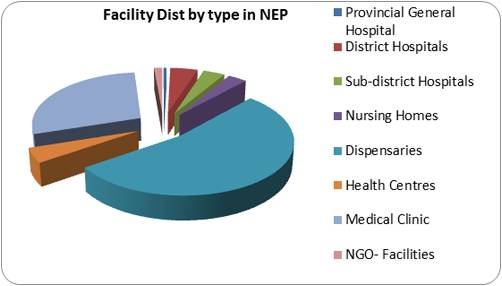
The average facility/population coverage rate for hospitals, health centers and
dispensaries in NEP is: 121,000, 230,000 and 19,000 respectively. While the
vertical distribution of these facilities may be right for the referral
framework, less than 42% people in this far-flung region have access to health
care: Geographical in-access stems from a mal-distribution of the facilities
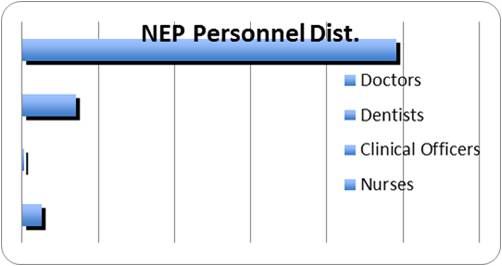
rather than the actual numbers (Fig. 7; Appendix. 2). NEP’s personnel
distribution is also significantly below its population share (Fig. 8), which
can be explained by personnel flight from the harsh environment and the
prejudicial perception by the rest of the country that the area is a hostile
no-go zone. Meanwhile, NEP lacks skilled locals to take over the vacant posts. |
|
-
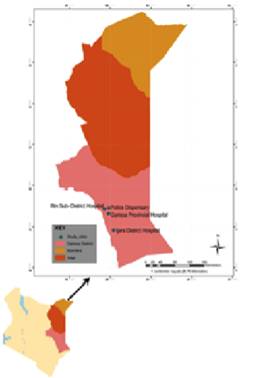 -
North Eastern Province, Kenya
|
|
|
|
|
Facilities Distribution by type in NEP |
|
|
|
|
|
|
|
|
|
|
|
 |
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Facilities Distribution by type in NEP |
Personnel Distribution NEP |
|
|
|
Source Ministry of Health, Division of Health Management Information System
(HMIS) |
|
|
|
|
|
|
|
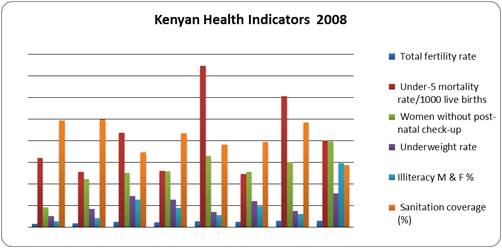
With poverty, education and health being interlinked, NEP has some of the
poorest heath indicators in the country. The province has the highest Total
Fertility Rate, women without postnatal check up, underweight rates, lowest
sanitation coverage and highest illiteracy amongst adults of both genders in the
whole country
|
|
|
|
 |
|
Such underserved populations would be the greatest beneficiaries of disease
surveillance programs like the USAMRD-K DEID AFI surveillance. AFI is a common
cause of morbidity and mortality in developing countries and a common complaint
in patients seeking medical attention in NEP. Infections continue to be its most
important cause but these remain poorly characterized in many parts of the world
largely due to limited diagnostic ability and the little active surveillance.
“High fever infections are so common here but we have no idea why or what the
causes are,” explains Dahaba. |
|
Source Kenya Demographic Health Survey 2008-2009 and HIMS annual report 2008. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Such underserved populations would be the greatest
beneficiaries of disease surveillance programs like the USAMRD-K DEID AFI
surveillance. AFI is a common cause of morbidity and mortality in developing
countries and a common complaint in patients seeking medical attention in NEP.
Infections continue to be its most important cause but these remain poorly
characterized in many parts of the world largely due to limited diagnostic
ability and the little active surveillance. “High fever infections are so common
here but we have no idea why or what the causes are,” explains Dahaba.
The illness is a major public health challenge in peripheral health care systems
as the etiologies may be clinically indistinguishable leading to misdiagnoses
and underreporting. The available data’s insufficient to assess the prevalence
and relative importance of the infectious agents and disease burden, estimate
priorities for health resources or refine policy on the empiric management of
febrile patients. Nationally, while the burden of some infections (e.g.,
Malaria) is understood to be substantial, the significance of others (e.g.,
brucellosis and rickettsial diseases) remains unknown- appendix 1. With no
etiology-specific signs and symptoms, a lack of knowledge of the scope of local
pathogens and unavailability of accurate diagnostic testing, patients in NEP are
empirically treated for Malaria with the potential for increased morbidity and
mortality.
“It has been puzzling because when we look at these patients- clinically they
have all the signs and symptoms of Malaria but when we send them to the lab, the
blood smears turn up negative,” explains Ahmed Noor an AFI recruiting clinical
officer at Iftin Sub-district Hospital. Noor says they then just disregard the
laboratory results, “per his judgment, the clinician will either prescribe
anti-malarials or manage the pain and fever with paracetamol as he buys time for
a hopefully better blood smear” he continues “in that case we ask the patient to
come back in 3 or so days, however, if the smear turns out negative again but
the patient still has a persisting fever- we still wind up dispensing
anti-malarials anyway.”
Sentinel hospital-based studies performed over defined periods of time have
provided useful clinical and public health information in countries that lack
resources for long-term routine diagnostic testing. This approach has been used
in Sub-Saharan Africa and Southeast Asia to determine the relative importance
and antimicrobial susceptibility patterns of common pathogens, and to provide
clinical predictors in well-defined patient populations. Additionally,
application of these methods has resulted in the identification of emerging or
previously unrecognized pathogens among these populations.
Similarly, the AFI surveillance will systematically assess the etiologies of
infections in patients presenting with fever to several hospitals and health
centers in NEP. The targeted panel of pathogens for investigation is
arboviruses, tick-borne bacteria, and several zoonoses. High animal exposure,
wide consumption of unpasteurized dairy products and rare animal vaccination or
insecticide spraying are all factors that favor the spread of infectious
diseases and the occurrence of simultaneous or multiple zoonoses. Additionally,
the common Somali shelter, the aqal, a dome-shaped, collapsible hut made from
poles covered by hides and woven fiber mats, while being flexible enough for the
nomads to carry on a camel’s back, is too exposed allowing easy entry of diverse
disease vectors.
NEP’s disease patterns are further complicated by a refugee population the
United Nations High Commission for Refugees (UNHCR) puts at 400,000 and a
further monthly influx of sometimes as high as 5,000 refugees. This is bound to
have an impact on the region as the vaccine coverage in Somalia is compromised
by the war; indeed, the World Health Organization (WHO) has previously reported
Polio outbreaks in the refugee camps. “There are so many diseases coming from
the other side”, says Noor, “before the surveillance we had no hope of knowing
what sort of diseases to expect, but with DEID coming in they have simplified
our work.”
The provision of accurate epidemiologic data for common pathogens will be of
practical importance to clinicians as the presence of infections for which
specific antimicrobial therapies are available might be identified. Where
microbiologic facilities cannot be permanently established, validated clinical
predictors may help guide therapeutic interventions. This has both Dahaba and
Noor excited, “with the DEID results streaming in, it will make patient
management informed” she says, while Noor adds, “patient mismanagement will be a
thing of the past.”
Dahaba explains additional benefits to clinicians “the fact that you are giving
us results from other AFI sites in the country is great for us because if we are
transferred elsewhere we will know what diseases to expect” she continues “DEID
is also training our lab staff on diagnosis and they have now become resource
persons to the other technicians around the hospital.” The surveillance
information will also enable targeted public health measures as resources can be
directed towards prevention of the diseases with the heaviest burden and in case
of outbreaks and epidemics.
However, though Dahaba can easily see the advantages of the project, it was not
received with jubilation by the wary and suspicious residents. “Most of our
people are illiterate and it takes time to convince them, they need more
enlightment on the project but slowly you will gain their trust,” she explained.
She however had a message of encouragement saying, “the initial suspicion that
was there is slowly ebbing due to the feedback we are getting from DEID and the
evident improvement of our lab staff performance since the project begun.”
Though the road has not always been smooth for AFI Somalia, the project has
grown from strength to strength. This July saw the initiation of the 2nd site-
the Police-line Health Center with a total of 8 field staff at both sites. This
has boosted sample numbers and more residents are buying into the idea. 2011
will see AFI Somalia expand to the larger NEP with additional sites in Ijaara
and Wajir districts.
|
|
As influenza viruses continue to evolve, attain more virulence and cross species
adaptability, surveillance serves as an important alert mechanism. |
|
|
|
THE REGIONAL INFLUENZA
SURVEILLANCE PROGRAMS
|
|
|
|
-
 -
The National Influenza team at the
center for public health research, Nairobi.
|
Influenza viruses continue to be very unpredictable, with the recent unexpected
triple re-assortant 2009 pandemic Flu A H1N1. Its quick spread across the globe
and the time it took for vaccines to be available is further proof that the
world is unprepared and vulnerable for a serious and more virulent influenza
pandemic. Nevertheless, the ability of the different countries to provide rapid
diagnosis including many developing countries with limited resources has been
impressive, this can be attributed to the previous H5N1 scare that enabled
better preparedness among nations.
|
|
-
 -
DEID field team identifying bird species and ringing
them to identify recaptured birds in avian influenza surveillance.
|
As influenza viruses continue to evolve and attain more virulence and cross
species adaptability, it is important to undertake surveillance as an alert
mechanism, to effect timely preventive and control mechanisms in case of the
emergence of influenza viruses that may be of pandemic potential. Starting with
Kenya, the USAMRD-K DEID influenza surveillance has now expanded to include,
Uganda, Tanzania and Cameroon. These surveillance activities are part of the
AFHSC-GEIS laboratory based influenza surveillance network around the world. It
serves the following goals of the DEID program:
• Detect local influenza outbreaks,
• Provide isolates for the WHO vaccine pool for vaccine component determination
that protects not only the US forces in foreign missions but also the general
public and to,
• Detect any emerging strains that could have pandemic potential. This is not
only important for the AFHSC-GEIS but also to the general public of the host
nations, the region and the scientific community in general.
|
|
|
|
|
|
 MHK’s mission is to provide microbiology expertise and laboratory support for
the detection and diagnosis of causes of acute diarrhea in Kenya. MHK’s mission is to provide microbiology expertise and laboratory support for
the detection and diagnosis of causes of acute diarrhea in Kenya. |
|
|
|
|
|
THE KENYAN HUMAN INFLUENZA SURVEILLANCE PROGRAM
-
 -
Human Influenza sampling sites in Kenya.
|
|
Prior to 2006, Kenya lacked
the laboratories and public health infrastructure to conduct sustained
influenza/influenza-like-illness surveillance (ILI). In 2006, DEID funded a
program to start conducting influenza surveillance in Kenya. The objective of
the program is to carry out sentinel surveillance for human influenza and ILI in
Kenyan outpatient clinics. The program has grown through the years, and the
AFHSC-GEIS funded National Influenza Center is now a major component in the
Kenyan Public Health infrastructure, serving not only Kenya but also, the
Republics of Seychelles and Somalia.
In brief, nasopharyngeal swabs are collected from patients presenting with
fever, cough or sore throat and the samples are transported weekly to the NIC
for analysis. Currently the NIC is able to carry out molecular and serologic
influenza diagnostics, isolation of viruses, characterization of their antigenic
properties and even mapping of their genetic changes that are indicative of
changes in virulence/antigenicity/drug resistance. However, the center plans to
develop the capacity to carry out all aspects of influenza testing to include in
vitro antiviral resistance testing to enable phenotypic drug characterization of
these viruses.
Furthermore, with the acquisition of a genetic analyzer in the summer of 2010,
it is envisioned that we will not only sequence Influenza but also look at the
other respiratory viruses being isolated in the laboratory. This capacity should
also benefit other local DEID laboratories (such as, the VHF & Arbovirology lab,
the avian influenza program, West Nile program, AFI program) as well as support
our regional collaborators in Uganda, Tanzania and Cameroon, improving existing
collaborations within and outside of the USAMRD-K DEID network.
For the immediate present, current influenza surveillance activities will be
sustained by continuous sample collection at the eight public hospitals and the
two KDoD facilities. We will also set up a committee within the laboratory that
will be tasked with writing manuscripts from the much data that has been
generated by the program thus improving it’s current publication output. In the
future, we hope the following activities will steer the program forward: An
increased collaboration with the KDoD; Expanding the influenza agenda beyond
surveillance and response activities, to include basic science research themes
with proposals focusing not only in on influenza but on other respiratory
viruses as well. The goal is to set up a regional centre of excellence in
respiratory virology in line with the AFHSC-GEIS mandate, vision and mission.
|
-
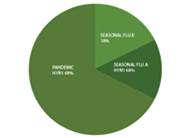 -
Pandemic H1N1 is the predominant strain in circulation in Kenya (Sep 09 – Mar
10).
|
|
|
|
Partners |
|
|
|
• Kenya Medical Research Institute (KEMRI)
• Kenya Ministry of Public Health and Sanitation (KMoPHS)
• CDC-Kenya (Global Disease Detection Program)
• United States Air Force School of Aerospace Medicine
(USAFSAM)
• Naval Health Research Centre (NHRC)
• Lovelace Respiratory Research Institute (LRRI) |
INFLUENZA VIRUSES SURVEILLANCE IN MIGRATORY BIRDS
-
 -
A plover bird trapped in a mist net
ready for sampling.
|
|
The U.S. Army Medical Research Directorate-Kenya, CDC-Kenya, the Kenya Medical Research
Institute, the National Museums of Kenya, the Kenya Ministry of Livestock
Development, and the U.S. Naval Medical Research Unit No 3, Egypt, began
collecting and testing migratory bird samples in 2005. Birds are trapped using
mist nets and cloacal and oropharyngeal swabs collected and stored in liquid
nitrogen in the field. Samples are screened for Influenza A and H5 subtype by
real time RT-PCR at laboratories either at CDC-Kenya, Nairobi or at NAMRU-3,
Egypt.
From October 2005 to June 2009 specimens from 3,618 birds representing 150 bird
species were collected in 13 sites with the majority of the specimens being
collected from sandpipers, plovers and ducks.
|
|
-
 The mass death of flamingoes in
Kenya in 2006 was attributed to a bird influenza outbreak.
|
|
Influenza A virus was detected in 1.7% (61/3618) of all the birds representing
23 different species. Of the 61 Influenza A virus positives 21(34%) were from
resident birds, 21(34%) from paleartic migrants and 19 (32%) from intra African
migrants. All the positives were detected during the migration period between
October- April. No positives were detected outside the migration period. No
highly pathogenic avian influenza viruses were detected during the study period.
However, 1 low pathogenic avian influenza virus (LPAI) H12N2 and 4 LPAI H5
subtypes whose neuraminidase subtype could not be established was detected in 4
bird species representing both resident and migratory species sampled in 3
sites.
Click on the image to enlarge and open in a new window. The discovery of
influenza viruses in both migratory and resident birds reinforces the
probability of the potential transmission between migratory and resident birds.
This effort has built local capacity for the expert collection and analysis of
bird influenza and has given animal and public health experts baseline
statistics of influenza virus activity in birds during the most recent, four
seasons. This surveillance has the potential to function as an early warning
system for Highly Pathogenic Avian Influenza.
|
|
|
|
The road side markets source poultry from all over the country, so this Live
Bird Market (LBM) preliminary study will give us a snapshot of bird flu
incidences in the whole country. |
|
|
|
|
|
|
DOMESTIC AVIAN INFLUENZA SURVEILLANCE |
|
|
|
-
 Mr.
Charles Magiri a DEID field coordinator bleeding a chicken for avian influenza
analysis.
|
Viruses of the Influenza A genus affect a variety of animals, especially birds
and pigs. Mixing of these viruses does sometimes lead to the emergence of new
influenza virus lineages that acquire the ability to infect and be transmitted
among the human population. To date, 16 HA and 9 NA subtypes of Influenza A
viruses have been identified, and all of these subtypes have been isolated from
avian species. The domestic avian influenza study seeks to initiate surveillance
of zoonotic influenza viruses in domestic poultry sold at live bird markets, and
eventually in humans who handle these birds |
-
 DEID
field team preparing cool boxes to transport the avian samples to the laboratory
for analysis.
|
The project begun in 2009 as a collaboration between DEID and the Department of
Veterinary Services (DVS) at the Ministry of Livestock and Animal Husbandry in
Kenya. Training on assays for assessing risk of exposure to zoonotic influenza
viruses was initiated at the Center for Emerging Infectious Diseases; Iowa State
University. Follow up visits from the Iowa University team to KEMRI and DVS
laboratories reinforced assay methodology and cohort study implementation. In
2010, DEID started a pilot study with a sample size of 500 birds at the LBMs.
Dr. David Ojigo of the DVS who often accompanied the field team explains “the
roadside markets source poultry from all over the country so this LBM
preliminary study will give us a snapshot of bird flu incidences in the whole
country.”
The
field team would operate from a ‘mobile poultry clinic’, the traders identify
the different locations where the birds were sourced. Blood samples, cloacal and
oral pharyngeal viral swabs from healthy birds as well as those with signs and
symptoms of influenza infection were collected and transported to the USAMRD-K
DEID laboratories in cool boxes for sorting and analysis. “The pilot study will
establish baseline statistics for further focused research,” says Dr. Ojigo.
While a majority of the traders were open to having their birds sampled, the
field team did not have it easy with all of them. “The resistance from traders
came from fear that the sampling could arouse suspicion from buyers who might
think the birds are sick which would drive down sales,” explains Mr. Charles
Magiri, the study’s field coordinator.
Ms. Veronica Nduku a 54-year-old trader has been in the chicken business since
1977. Today, she sells her chicken at stalls along the busy Jogoo Road. Veronica
is one of the supportive traders, she says, “we had been selling birds for a
long time and had never before heard about this disease (avian influenza), then
suddenly, there were media announcements that the birds were sick and our sales
plummeted.” Continues Veronica, “I welcomed this project because we can now
understand bird flu better, additionally, when surveillance is going on, it is
easier to detect other diseases that might arise faster as the structures will
already be in place.”
In the laboratory viral RNA template was prepared and later used in a Multiplex
PCR for detection of gene targets for multiple influenza subtypes (H1, H2, H3,
H5, H7, H9, N1 and N2). Amplicons will be sequenced and compared to existing
wild type sequences. The traders who appreciate the benefit of the study say
they are really happy that the government is also showing that they not only
care for the big beef industry but for the small-scale poultry traders as well.
A human-use protocol will be written during the 1st quarter, FY 2011 to allow
identification of viruses at the bird-human inter-phase. Veronica says it will
be really beneficial to sample the traders, “sometimes we have respiratory
illnesses that we suspect could be related to our occupation,” she explains. The
surveillance data emanating from this project will be valuable in establishing
the role domestic chicken play in the continued evolution of influenza viruses
and the best strategy for effective control. This is a critical area to the DEID
program, and the world at large especially in the wake of the current H1NI
outbreak.
 |
|
|
With the widespread resistance to flouroquinolones and rapidly changing drug
sensitivity profile of N. genorrhea in other parts of the world, it is prudent
for Kenya to undertake surveillance to monitor N. genorrhea antimicrobial
resistance. |
|
|
GONORRHEA DRUG SUSCEPTIBILITY SURVEILLANCE
-

Antimicrobial Susceptibility E test.
|
Generally, sexually transmitted infections (STIs) associated with discharge like
gonorrhea are a serious health problem in Kenya. However, available data on STIs
caused by Neisseria gonorrhoeae in Kenya are limited though high prevalence of
gonorrhea has been reported in special risk groups in both urban and rural
populations. Patients presenting to Ministry of Health (MoH) clinics with
complaints suggestive of STIs often go undiagnosed, and are treated empirically
with broad spectrum antibiotics in line with the WHO recommendations for
syndromic management of STIs. |
-
Streaks of N. gonorrhea isolates.
|
Treatment consists of fluoroquinolones such as Norfloxacin prescribed together
with an antibiotic usually doxycycline or azithromycin. With the widespread
increase in resistance to fluoroquinolones and a rapidly changing drug
sensitivity profile of N. gonorrhoeae in other parts of the world, it is prudent
for Kenya to undertake surveillance to monitor N. gonorrhoeae antimicrobial
resistance as part of a comprehensive prevention strategy that should also adapt
screening recommendations for individuals at high risk for infection, and assure
prompt and effective treatment for infected persons and their sexual partners.
The surveillance of antimicrobial susceptibility profiles of Neisseria
gonorrhoeae isolates from patients seeking treatment in select military and
civilian clinics in Kenya is a new project under the DEID STI program. The aim
of the study is to establish and monitor antimicrobial susceptibility profiles
of N. gonorrhoeae isolates from patients seeking treatment for sexually
transmitted diseases in these facilities. Surveillance activities under this
project will involve recruitment of patients presenting with STIs suggestive of
gonorrhea, enrollment of patients who are rapid test positive for gonorrhea and
isolation of N. gonorrhoeae for antimicrobial susceptibility testing.
Isolates of N. gonorrhoeae obtained from patients will be used for antimicrobial
susceptibility testing using the E-test method to determine the minimum
inhibition concentrations of a selection of the antimicrobial agents recommended
for treatment of gonorrhea. Antimicrobial susceptibility testing will be done at
the USAMRD-K- DEID Centre for Microbiology Research Laboratory in KEMRI,
Nairobi.
|
-

Dr. Margaret Mbuchi prepares agar dilutions for N.
gonorrhea anti-microbial susceptibility testing.
|
It is hoped that data arising from this surveillance will shed light on the
extent of gonococcal antimicrobial resistance in Kenya, and also provide a
rational basis for recommended treatment regimens. This data will also play a
crucial role in guiding therapy and combating drug resistance. The protocol for
the study which has already been reviewed and approved by the WRAIR scientific
committee and the Department for Human Subject Protection has recently been
approved by the KEMRI/National Ethics Review Committee and is scheduled to
initially start in two civilian sites in the month of January, 2011. |
|
|
Partners |
|
|
|
• Kenya Ministry of Defence (KDoD)
• University of Washington (UW)
• Kenya Ministry of Public Health and Sanitation
 Kenya,
an epicenter of Malaria drug resistance emergency in Africa continues to
experience significant malaria-related morbidity and mortality. Kenya,
an epicenter of Malaria drug resistance emergency in Africa continues to
experience significant malaria-related morbidity and mortality. |
|
|
|
|
|
|
|
|
|
|
|
|
Publications
1. NEW Peter Obare, Bernhards Ogutu, Mohammed Adams, James Sande Odera, Ken
Lilley, David Dosoo, Christine Adhiambo, Seth Owusu-Agyei, Fred Binka, Elizabeth
Wanja and Jacob Johnson Misclassification of Plasmodium infections by
conventional microscopy and the impact of remedial training on the proficiency
of laboratory technicians in species identification. Virology Journal 2013,
10:140. View the Publication
2. NEW Caroline Ochieng, Joel Lutomiah, Albina Makio, Hellen Koka, Edith
Chepkorir, Santos Yalwala, James Mutisya, Lillian Musila, Samoel Khamadi, Jason
Richardson, Joshua Bast, David Schnabel, Eyako Wurapa and Rosemary Sang.
Mosquito-borne arbovirus surveillance at selected sites in diverse ecological
zones of Kenya, 2007 – 2012; Virology Journal 2013, 10:140.
View the Publication
3. NEW Fredrick L. Eyase, Hoseah M. Akala, Luiser Ingasia, Agnes Cheruiyot,
Angela Omondi, Charles Okudo, Dennis Juma, Redemptah Yeda, Ben Andagalu,
Elizabeth Wanja, Edwin Kamau, David Schnabel, Wallace Bulimo, Norman C. Waters,
Douglas S. Walsh, Jacob D. Johnson, The Role of Pfmdr1 and Pfcrt in Changing
Chloroquine, Amodiaquine, Mefloquine and Lumefantrine Susceptibility in
Western-Kenya P. falciparum Samples during 2008–2011, PLOS One 2013.
View the
Publication
4. NEW Victor O. Ofula, Alan B. Franklin, J. Jeffrey Root, Heather J. Sullivan,
Patrick Gichuki, Albina Makio, Wallace Bulimo, Bernard O. Abong’o, Muchane
Muchai, and David Schnabel, Detection of Avian Influenza Viruses in Wild
Waterbirds in the Rift Valley of Kenya Using Fecal Sampling, Vector-borne and
Zoonotic Diseases, Journal Volume 13, Number X, 2013.
View the Publication
5. NEW Ismail Mahat Bashir, Nekoye Otsyula, George Awinda, Michele Spring, Petra
Schneider, John Njenga Waitumbi. Comparison of PfHRP-2/pLDH ELISA, qPCR and
Microscopy for the Detection of Plasmodium Events and Prediction of Sick Visits
during a Malaria Vaccine Study. PLOS ONE Journal, 2013.
View the Publication
6. NEW Denis K Byarugaba, Bernard Erima, Monica Millard, Hannah Kibuuka, Lukwago
L, Josephine Bwogi, Derrick Mimbe, Edison A Mworozi, Bridget Sharp, Scott
Krauss, Richard J Webby, Robert G Webster, Samuel K Martin, Fred Wabwire-Mangen
and Mariette F Ducatez. Genetic analysis of influenza B viruses isolated in
Uganda during the 2009–2010 seasons. Virology Journal 2013, 10:11.
View the
Publication
7. NEW E. Okoth, C. Gallardo, J.M. Macharia, A. Omore, V. Pelayo, D.W. Bulimo,
M. Arias, P. Kitala, K. Baboon, I. Lekolol, D. Mijele, R.P. Bishop. Comparison
of African swine fever virus prevalence and risk in two contrasting pig-farming
systems in South-west and Central Kenya, PREVET (2012).
View the Publication
8. NEW Karen K. Wong, Wallace D. Bulimo, Japhet Magana, Rachel A. Achilla,
Sandra K. Schwarcz, Maylor Simwa, Janet M. Majanja, Meshack O. Wadegu, Finley A.
Osuna, Silvanos O. Mukunzi, Josephat K. Mwangi, Julia M. Wangui, Janet N.
Muthoni, James O. Njiri, Beryl D. Obura, Benjamin H. Opot, Keneth K. Mitei, Jane
Barani, Samwel Lifumo, and David C. Schnabel. Epidemiology of 2009 Pandemic
Influenza A Virus Subtype H1N1 Among Kenyans Aged 2 Months to 18 Years,
2009–2010, J Infect Dis. (2012) 206(suppl 1): S68-S73 doi:10.1093/infdis/jis585.
View the Publication |
Download the PDF |
View the Abstract
9. NEW Clayton O. Onyango, 1 Regina Njeru, 1 Sidi Kazungu, 1 Rachel Achilla, 2
Wallace Bulimo, 2 Stephen R. Welch, 3 Patricia A. Cane, 3 Rory N. Gunson, 6
Laura L. Hammitt, 1,4 J. Anthony G. Scott, 1,4 James A. Berkley, 1,4 and D.
James Nokes 1,5 Influenza Surveillance Among Children With Pneumonia Admitted to
a District Hospital in Coastal Kenya, 2007–2010.
View the Publication |
Download
the PDF |
View the Abstract
10. NEW Wallace D. Bulimo; Rachel A. Achilla; Janet Majanja; Silvanos Mukunzi;
Meshack Wadegu; Finnley Osunna; Josephat Mwangi; James Njiri; Julia Wangui;
Janet Nyambura; Beryl Obura; Ken Mitei; Duke Omariba; Shirley Segecha; Martha
Nderitu; Alfred Odindo; Charles Adega; Jeremiah Kiponda; Ruth Mupa; Frida
Munyazi; George Kissinger; Mohammed Mwakuzimu; Diana Kamola; Elias Muhidin;
Daniel Kamau; Steve Kairithia; Margaret Koech; Alice Sang; Lynette Onge'ta;
David C. Schnabel. Molecular Characterization and Phylogenetic Analysis of the
Hemagglutinin 1 Protein of Human Influenza A Virus Subtype H1N1 Circulating in
Kenya During 2007-2008. Journal of Infectious Diseases 2012 206: S46-S52.
View
the Publication |
Download the PDF |
View the Abstract
11. Wallace D. Bulimo, Silvanos Mukunzi, Rachel Achilla, Benjamin H. Opot,
Finley Osuna, Janet Majanja, Meshack Wadegu, and Eyako K. Wurapa. Were the
WHO-recommended Human Influenza Vaccine formulations appropriate for Kenya
during the 2010-2011 Season? Inferences from the HA1 Gene Analysis. African
Journal of Pharmacology and Therapeutics Vol. 1 No. 2 Pages 46-54, 2012.
View
the Publication
12. Wallace D. Bulimo, George Gachara, Benjamin H. Opot, Margaret W. Murage and
Eyako K. Wurapa, 2012. Evidence in Kenya of reassortment between seasonal
influenza A(H3N2) and influenza A(H1N1)pdm09 to yield A(H3N2) variants with the
matrix gene segment of A(H1N1)pdm09. Afr. J. Pharmacol. Ther. 1(1): 1-7.
13. An Investigation of a Major Outbreak of Rift Valley Fever in Kenya:
2006-2007 Patrick M. Nguku, S. K. Sharif, David Muton- ga, Samuel Amwayi, Jared
Omolo, Omar Mohammed, Eileen C. Farnon, L. Hannah Gould, Edith Lederman, Carol
Rao, Rosemary Sang, David Schnabel, Daniel R. Feikin, Allen Hightower, M. Kari-
uki. Njenga, and Robert F. Breiman Am J Trop Med Hyg 2010; 83 05-13.
14. Rift Valley Fever Virus Epidemic in Kenya, 2006/2007: The En- tomologic
Investigations Rosemary Sang, Elizabeth Kioko, Joel Lutomiah, Marion Warigia,
Caroline Ochieng, Monica O'Guinn, John S. Lee, Hellen Koka, Marvin Godsey, David
Hoel, Hanafi Hanafi, Barry Miller, David Schnabel, Robert F. Breiman, and Ja-
son Richardson Am J Trop Med Hyg 2010; 83 28-37.
15. Prediction, Assessment of the Rift Valley Fever Activity in East and
Southern Africa 2006-2008 and Possible Vector Control Strategies: Assaf Anyamba,
Kenneth J. Linthicum, Jennifer Small, Seth C. Britch, Edwin Pak, Stephane de La
Rocque, Pierre For- menty, Allen W. Hightower, Robert F. Breiman, Jean-Paul
Chre- tien, Compton J. Tucker, David Schnabel, Rosemary Sang, Karl Haagsma, Mark
Latham, Henry B. Lewandowski, Salih Osman Magdi, Mohamed Ally Mohamed, Patrick
M. Nguku, Jean-Marc Reynes, and Robert Swanepoel Am J Trop Med Hyg 2010;83
43-51.
16. Outpatient Upper Respiratory Tract Viral Infections in Children with Malaria
Symptoms in Western Kenya. Accepted in the Am J Trop Med Hyg.Waitumbi John, Jane
Kuypers, Samuel B. Anyona, Joseph N. Koros, Mark E Polhemus, Jay Gerlach,
Matthew Steele, Janet A Englund, Kathleen M Neuzil, Gonzalo J Domingo.
17. Waitumbi John, Jay Gerlach, Irina Afonina, Samuel B. Anyo- na, Joseph N.
Koros, Joram Siangla, Irina Ankoudinova, Mitra Singhal, Kate Watts, Mark E
Polhemus, Nic Vermeulen, Walt Mahoney, Matt Steele, Gonzalo J Domingo. Malaria
prevalence defined by microscopy, antigen detection, DNA PCR and total nucleic
acid PCR in a malaria endemic region during the peak malaria transmission
season. Submitted to the Am J Trop Med Hyg.
18. Woodring JV, Ogutu B, Schnabel D, Waitumbi JN, Olsen CH, Walsh DS, Heppner
DG Jr, Polhemus ME. Evaluation in the recur- rent parasitemia after
artemether-lumefantrine treatment for uncomplicated malaria in children in
western Kenya. Am J Trop Med Hyg. 2010 Sep; 83(3): 458-64. 19. Jeremy Sueker et
al. (2010).Influenza and Respiratory disease surveillance: the US military’s
global laboratory based network. Influenza and other respiratory diseases: 4
(3), 155-161.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|